Persistent post-concussion symptoms aren't always a brain problem.
When the head decelerates fast enough to concuss the brain, the upper cervical spine experiences the same forces. The atlas and axis are the smallest, most mobile bones in the spinal column, sitting at the end of a heavy lever (the head) attached by ligaments designed for precision, not impact absorption. When concussion mechanics happen, from whiplash, sports collision, a fall, or a motor vehicle accident, the joint structure where the skull meets the spine is frequently disrupted alongside whatever happened inside the brain.
In the acute phase, the brain injury dominates the clinical picture. Patients get the right care: cognitive rest, graduated return to activity, vestibular rehab if needed, neurology follow-up. Most concussions resolve within two to four weeks.
The ones that don't, the patients who sit at three months, six months, two years post-injury, still cycling through brain fog, headaches, autonomic instability, sleep disruption, exercise intolerance, are who this article is for.
In a significant fraction of post-concussion syndrome cases, the persistent symptoms aren't being generated by ongoing brain pathology. They're being generated by an upper cervical injury that was never addressed.
What gets missed in the standard post-concussion workup
The standard workup for persistent post-concussion symptoms looks at the brain. Neurology evaluation. Cognitive testing. Vestibular and ocular-motor screening. Sometimes neuroimaging, though imaging is usually unrevealing in mild TBI. Treatment focuses on symptom management, cognitive rehabilitation, and graduated exercise progression under expert guidance.
What's usually not in the workup is a structural assessment of the upper cervical spine. The neck might get a cursory range-of-motion check. Soft tissue tension might be palpated. But the specific question, is there a mechanical disruption at the top of the neck that's driving the autonomic and proprioceptive dysfunction we're seeing, usually doesn't get asked, because the providers in the standard workup aren't trained to assess it.
This isn't a criticism of those providers. It's a gap. Concussion care developed within neurology and rehabilitation medicine, and the upper cervical spine sits at the intersection of orthopedics, neurology, and chiropractic. None of the standard workup specialists own that real estate.
The result is a category of post-concussion patients whose persistent symptoms are largely or entirely cervicogenic, and who've been told for months or years that their brain is the problem.
In short: Concussion forces don't stop at the skull. The upper cervical spine absorbs the same impact, and structural injury there can persist long after brain healing is complete. When persistent post-concussion symptoms don't respond to standard care, the upper cervical assessment is often the missing piece.
Why the upper cervical spine matters in concussion
Three mechanisms link upper cervical injury to persistent post-concussion symptoms.
The first is proprioceptive. The suboccipital region is the densest proprioceptive structure in the spine. When that input becomes distorted by joint misalignment or chronic muscle compensation, the brainstem receives noisy position signals. The resulting symptoms (dizziness, balance disruption, visual processing issues, neck-eye coordination problems) overlap almost exactly with the symptoms attributed to post-concussion vestibular dysfunction. Cervical input and vestibular input converge at the same brainstem region. Distorted cervical input produces vestibular-type symptoms even when the inner ear itself is intact.
The second is autonomic. The vagus nerve passes through the upper cervical region. The sympathetic chain has dense innervation in the cervical spine. When the structural environment at the top of the neck is disrupted, autonomic regulation often becomes dysregulated. This shows up as heart rate variability collapse, orthostatic intolerance, temperature dysregulation, GI symptoms, sleep architecture disruption, and exercise intolerance. The constellation gets labeled "post-concussion autonomic dysfunction," but it doesn't always have a brain-side driver.
The third is biomechanical. Persistent neck pain after concussion is common. Persistent neck pain alters movement patterns. Altered movement patterns drive further compensation. The patient becomes a person whose head doesn't move freely on the neck, whose neck doesn't move freely on the shoulders, and whose nervous system is constantly managing the compensation. That cost shows up as fatigue, headache, and reduced cognitive bandwidth.
Address the structural injury, and the proprioceptive, autonomic, and biomechanical cascades often unwind together.
Why Atlas Orthogonal specifically
The post-concussion population is a high-stakes group to treat. Standard rotational chiropractic adjustment, high-velocity, low-amplitude thrust with a rotational component, is contraindicated in many post-concussion cases, particularly those with ligamentous injury, vascular concerns, or significant autonomic dysregulation. Forceful manipulation can worsen symptoms or, in rare cases, cause harm.
Atlas Orthogonal is mechanically distinct from rotational chiropractic. The correction is delivered through a percussion instrument calibrated to deliver a specific, low-amplitude force vector. No rotation. No thrust. The patient lies on their side with the head supported on a stylus positioned based on precise upright imaging.
For the post-concussion population, this matters. The force profile is sub-clinical for ligamentous injury, vascular structures, and the autonomic system. It's appropriate to use in patients who would not be candidates for rotational manipulation.
This isn't a marketing point. It's a clinical reason AO has developed a niche in post-concussion care. The technique fits the population.
What the evidence shows
The strongest evidence linking upper cervical injury to persistent post-concussion symptoms comes from convergent clinical literature on whiplash-associated disorders. The mechanisms of whiplash and sport-concussion overlap substantially. The persistent symptom patterns overlap substantially. The biomechanical injury patterns at the top of the neck overlap substantially.
Schneider's work at the University of Calgary, published in British Journal of Sports Medicine (2014), demonstrated that combined cervical and vestibular rehabilitation outperformed standard care in adolescents with persistent post-concussion symptoms. The cervical contribution to recovery is now sufficiently established that the international consensus statements on concussion recognize cervical assessment as part of comprehensive post-concussion care.
What hasn't been studied directly is AO-specific outcomes in post-concussion populations. Case series exist. Clinical observation across the AO community is consistent: a meaningful fraction of persistent post-concussion patients respond to upper cervical correction when standard care has plateaued. The mechanistic logic is sound, the technique is appropriate for the population, and the response pattern is reproducible.
AO is not a treatment for traumatic brain injury. Brain injury rehabilitation is its own discipline. What AO can address, when present, is the upper cervical component that frequently accompanies and outlasts the brain injury itself.
What the assessment looks like
The first visit is a consultation and full assessment. It is not a treatment session. We do not adjust on the first visit, ever. For post-concussion patients specifically, this matters even more than usual. The autonomic system is often fragile post-injury, and the assessment process needs to respect that.
The visit covers history, physical examination, and the structural and autonomic assessment workup. Thermography maps sympathetic asymmetry in skin temperature. Surface EMG captures muscle activation patterns, particularly in the suboccipital and cervical paraspinal regions. Heart rate variability baselines your autonomic capacity, and that number often tells us how cautiously to proceed.
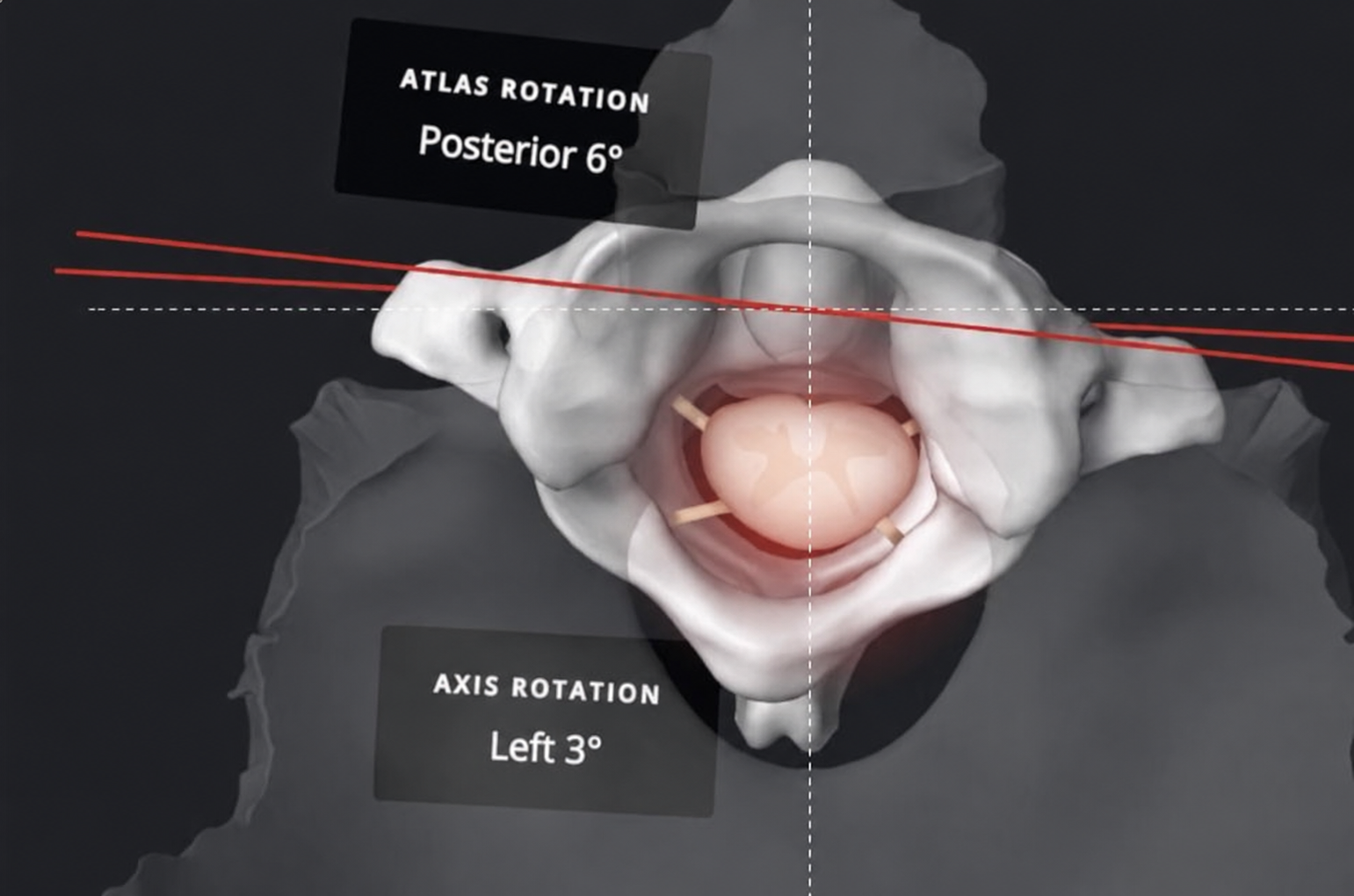
Every new patient gets upper cervical x-rays. Imaging is fundamental to the approach. The geometry of your alignment determines the corrective force vector for atlas orthogonal, and that geometry can only be measured from precise upright views. For post-concussion patients, the imaging is particularly important because we need to confirm there's no structural finding that contraindicates upper cervical work, and we need precise measurements to calculate a corrective approach gentle enough for the population.
Between the first and second visits, the doctor reviews everything: the imaging, the assessment data, the history. The corrective plan is calculated from the measurements.
The second visit is the report of findings. The doctor sits down with you, walks through what the imaging and assessment showed, explains the plan, and answers your questions. When the case is appropriate for upper cervical care, the first correction is delivered at this visit.
The correction itself is brief. You lie on your side. The instrument delivers a measured force. There's no thrust, no rotation, no audible cavitation. You rest for ten to fifteen minutes after. We reassess thermography and HRV.
You go home. You don't return the next day. The nervous system needs time to integrate. We typically reassess at 48 to 72 hours and space subsequent visits based on how the correction holds.
For acute post-concussion patients (within 6 weeks of injury), we coordinate with neurology and any vestibular rehab providers actively managing the case. For chronic patients (persistent symptoms 3+ months out), we're frequently the missing piece, but we're not the only piece. Concurrent care often includes vestibular PT, sleep medicine, autonomic specialists, or functional medicine depending on the symptom picture.
What to expect over time
Two things are true about post-concussion recovery with AO care, and they both matter.
The first: response can be fast. A meaningful percentage of post-concussion patients report immediate relief after the first correction. Brain fog clears within hours. A headache that's been constant for months breaks. Sleep deepens that night. Energy comes back the next morning. That immediate response is real, and it tells us the upper cervical component was driving a significant share of the symptom load.
The second: lasting recovery requires commitment to care. Immediate relief is the beginning of the process, not the end. The deep, sticky results — the ones where the autonomic dysregulation resolves and stays resolved, where exercise tolerance returns to baseline, where sleep architecture rebuilds, where the system feels integrated again — come from consistent follow-through across weeks and months. The nervous system needs repeated exposure to corrected structural input to reorganize. A single correction can produce relief. Sustained recovery comes from a treatment plan you finish.
Realistic timelines vary. Some patients see meaningful change within 4 to 6 visits over 6 to 8 weeks. Some take 3 to 6 months of consistent care to see the system fully reorganize. A small subset don't respond, which is the data point that tells us the persistent symptoms have a different driver. Sometimes a vestibular issue, sometimes a missed metabolic or psychiatric contributor, sometimes a structural problem outside our scope.
If your symptoms have an upper cervical driver, response shows up in the first 4 to 6 corrections. If we don't see meaningful change in that window, we're either wrong about the driver or there's something else going on that needs to be addressed. That's an honest framework for deciding whether to continue care.
When to seek other care
Concussion care is multidisciplinary by necessity. AO addresses one piece. It's not the whole picture for most patients.
If you have current red flags, worsening headache, repeated vomiting, new neurological deficits, escalating confusion, or seizure activity, that's a medical emergency. Emergency department first, AO never.
If you have ongoing vestibular symptoms that haven't been worked up by a vestibular specialist, that's a referral before AO. We work alongside vestibular PT, not instead of it.
If you have persistent cognitive symptoms (memory, executive function, processing speed) without addressing whether they're cervicogenic versus brain-driven, neuropsychological evaluation is part of due diligence.
If autonomic dysfunction is severe, POTS-level orthostatic intolerance, profound exercise intolerance, severe GI dysmotility, autonomic specialist involvement is appropriate alongside structural care.
Schedule your assessment
If standard post-concussion care has plateaued and persistent symptoms are still running your life months or years after injury, the upper cervical assessment is the piece that's usually missing.
The first visit is a consultation, full assessment, and imaging. The doctor reviews everything before your second visit and walks you through findings then. If your case has an upper cervical component worth treating, the corrective plan starts at visit two. If it doesn't, we'll tell you, and we'll point you where to go next.
Schedule your assessment today.
References